

Restoring nightly sleep architecture
Is it even helpful to know how much deep and REM sleep you are getting every night?

Last week, a reader from my article Why Your Sleep Score Sucks asked a question I suspect many wearable users have wondered too. And because I’m not a sleep expert by trade, I wanted to dig into the evidence before running off with my own opinion.
The question was really two-fold:
“I use an Apple Watch to track my sleep, and I’m a little dubious about how it divides my night into sleep stages. Does that matter? And is it actually helpful to know how much deep and REM sleep I’m getting every night?”
It’s a sharp question. And the evidence-based answer is: yes, but with nuance.
So let’s walk through the stages of nightly sleep, what a healthy hypnogram looks like compared with a fragmented one, and how to interpret your wearable data without spiraling every morning. I even made you a downloadable list of metrics worth paying attention to.
As any smart ring wearer will notice, sleep is a rhythmic state.
What might not be so obvious is that our brain cycles through four distinct stages about every hour and a half. And it does this four to five times each night.
These are rather fixed stages and are not interchangeable, meaning you cannot skip one stage and make up for it with extra time at the end. All the stages in your nightly sleep journey do something physiologically distinct and irreplaceable.
There are two stages of light sleep, a deep sleep stage, and, of course, the infamous REM (rapid eye movement) stage. Before I nerd out on the physiological processes in each of the stages, you might be wondering:
How important are sleep stages for health?
That answer, fortunately, is not nuanced. The science is clear on this one: yes, our sleep stages matter. Substantially.
In 2024, a landmark study in Nature Medicine tracked 6,785 participants who wore Fitbit devices for a median of 4.5 years. The collected data were cross-referenced with electronic health records, and the findings were striking: REM sleep and deep sleep were inversely associated with the odds of developing atrial fibrillation, and sleep duration, stage distribution, and irregularity were all independently associated with the incidence of obesity, cardiovascular disease, and psychological disorders [19].
This means that the more REM and deep sleep you get, the lower your odds of developing atrial fibrillation. Fewer of those stages = higher risk. More of those stages = lower risk.
The mechanistic picture is consistent with these population findings.
Deep sleep deprivation impairs immune function and hormone output, and glymphatic clearance (your brain's dedicated waste disposal network).
REM deprivation disrupts emotional regulation and cognitive integration.
Chronically fragmented sleep, where stages are interrupted before their functions are complete, compounds these deficits even when total sleep time appears adequate.
So that is the straight answer to the first question, “Do sleep stages matter?” Unequivocally, yes. But the second part of that question matters is where the nuance lies: …is it actually helpful to know how much deep and REM sleep I’m getting every night?
Let’s be nerdy about the fun physiology of sleep stages and get to the bottom of tracking nightly metrics.
Light Sleep: Stages N1 and N2
When you are snug and comfy in bed and close your eyes, you begin to drift into your first stage of sleep. This is appropriately named N1 and lasts only a few minutes. N1 is when the brain begins to disengage from the day and the environment; muscle twitches may occur, and we enter a deeper, more moderate light sleep called N2. The sleep scientists made this first part incredibly easy to remember. Thank you.
N2 is where the majority of light sleep occurs and where two highly specialized electrical events take place [12]:
Sleep spindles: brief bursts of neural oscillations
K-complexes: large bi-phasic waves that appear to serve a protective function, suppressing our attention so that deeper sleep can be maintained
Sleep spindles in particular are now understood to be critical for motor learning and procedural skill consolidation. Research has linked higher spindle density to better performance on tasks learned the previous day.
Light sleep is also the stage in which the brain transitions between deeper stages. Without adequate N2, sustained deep sleep and REM become harder to maintain. The National Sleep Foundation defines ideal sleep architecture as spending no more than 5% of the night in stage N1, and less than 81% in N2.
Deep sleep: Stage N3
This is our most physically restorative stage of sleep. The brain produces large delta waves in synchrony with one another, and our entire system shifts into repair and consolidation mode. The National Sleep Foundation defines ideal sleep architecture as spending 16–20% of sleep time in slow-wave sleep.
Deep sleep is front-loaded into the night. The first one to two sleep cycles contain the longest, deepest slow-wave sleep periods. By cycles four and five, the brain barely descends into deep sleep at all.
Several key processes converge across the deep sleep cycles:
Growth hormone release.
The majority of the day's growth hormone secretion occurs during deep sleep, not just for children, but throughout adult life. This hormone drives tissue repair, fat metabolic regulation, muscle recovery, bone density maintenance, immune function, and cellular regeneration. A chronic shortfall of deep sleep measurably reduces growth hormone output.
If you are cutting sleep short, drinking alcohol (which suppresses that first deep sleep block), or chronically getting fragmented sleep, you are systematically under-producing growth hormone night after night. Over the years, the cumulative effect on body composition, metabolic health, and tissue integrity is substantial.
Glymphatic clearance.
This is our brain’s dedicated waste-drainage network. Cerebrospinal fluid pulses through channels surrounding blood vessels, flushing out metabolic byproducts that accumulate during waking hours, including amyloid-beta and tau, both of which are associated with Alzheimer's disease [18].
A 2025 paper published in Cell identified the precise mechanism: norepinephrine levels oscillate in slow waves during NREM sleep, driving synchronized fluctuations in cerebral blood volume and CSF flow that power the clearance process [10].
A concurrent review confirmed that glymphatic insufficiency, caused by chronically poor deep sleep, is now implicated in the accumulation of neurotoxic proteins, including alpha-synuclein, relevant to Parkinson's disease [6].
Cardiovascular restoration.
Heart rate and blood pressure drop to their lowest levels of the day during deep sleep, giving the cardiovascular system a sustained period of reduced demand. This nightly dip is considered cardioprotective; people whose blood pressure fails to drop during sleep (a phenomenon called non-dipping) have significantly higher cardiovascular risk.
Memory consolidation.
Newly acquired facts and memories that you learned, experienced, or were told that day are replayed and transferred from the hippocampus to the neocortex for long-term storage. This process is why sleep deprivation so reliably impairs learning retention [16].
Immune system amplification.
Cytokines are molecules that coordinate the immune response, and their levels peak during deep sleep. This is one reason that sleep deprivation can impair vaccine response and immune function, and why febrile illness increases slow-wave sleep: the body is attempting to run its repair programs at higher intensity.
Because deep sleep stages lengthen as the night goes on, even a modestly shorter total sleep (losing the first or last 90 minutes) has very different consequences. Losing the beginning of sleep disproportionately costs deep sleep; losing the end costs REM.
REM sleep stage
The National Sleep Foundation defines ideal sleep architecture as spending 21-30% of the night in REM. This stage of sleep is neurologically extraordinary. The brain's metabolic rate and regional blood flow resemble those of the waking state, yet the body is functionally paralyzed, with voluntary muscles actively inhibited by the brainstem to prevent the physical enactment of dreams.
This is the time in dreams when we can’t seem to find our legs to sprint away from danger, or toward something we love. REM serves several functions that cannot be replicated by other stages:
Emotional memory processing.
The amygdala, our brain's primary emotional processing center, is highly active during REM, replaying emotional experiences in a neurochemical environment stripped of norepinephrine, the stress hormone. This is thought to allow the brain to re-encode emotional memories with reduced affective charge, essentially processing difficult experiences without retriggering the full stress response [3]. Chronic REM deprivation is associated with heightened emotional reactivity, worsened anxiety, and impaired trauma recovery.
Procedural memory and creativity.
Motor skill learning, pattern recognition, creative problem-solving, and insight (the ability to suddenly connect disparate pieces of information) all depend heavily on REM consolidation. The expression "sleep on it" is physiologically grounded: REM sleep reshuffles and integrates information in ways that waking cognition does not.
Emotional regulation for the coming day.
REM periods grow progressively longer across the night, with later cycles heavily REM-dominant, which is why the final one to two hours of sleep are disproportionately valuable for emotional regulation and cognitive function [16]. This is why people who regularly sleep six hours instead of eight often report heightened irritability, anxiety, and emotional dysregulation.
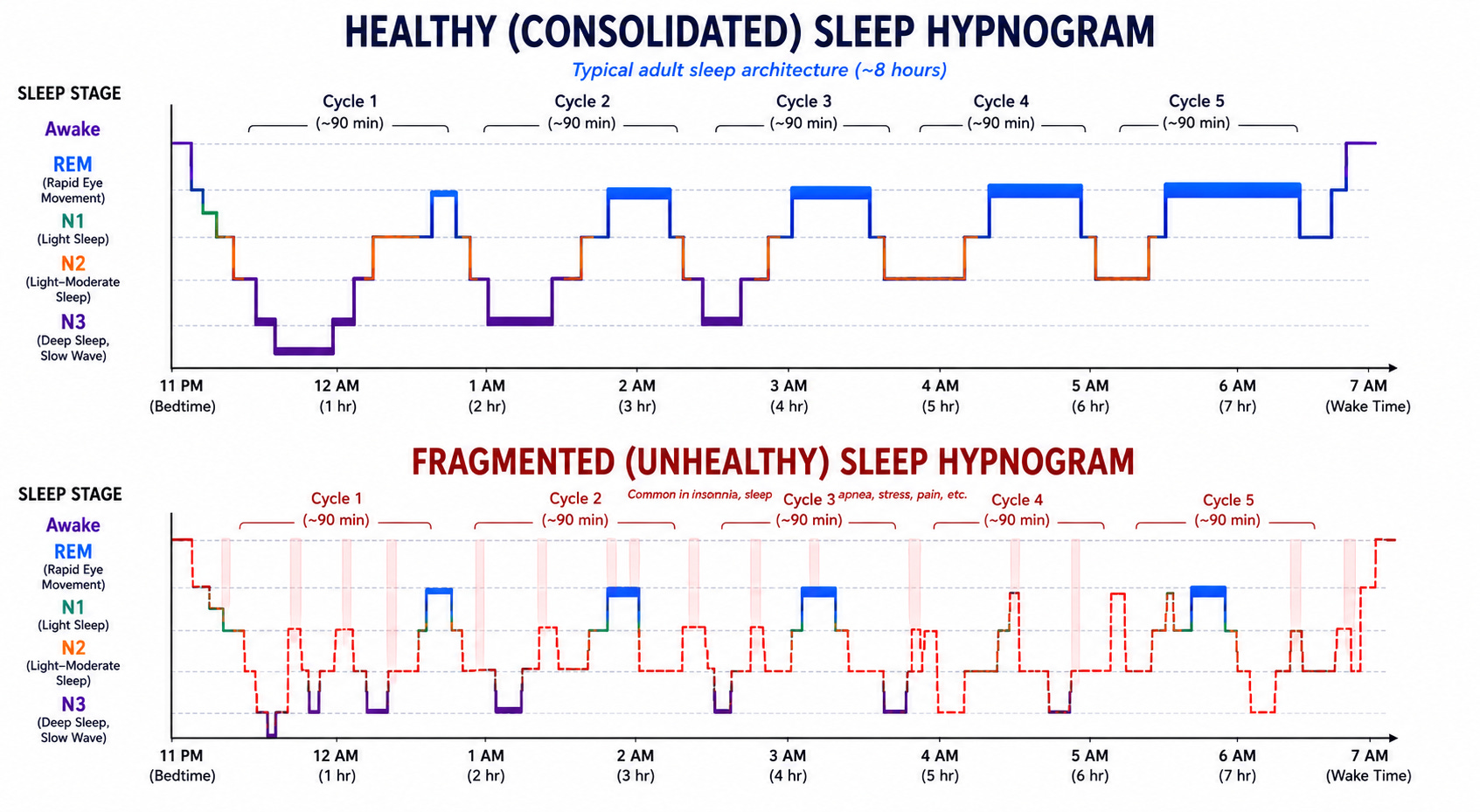
What a healthy sleep pattern versus a fragmented sleep pattern might look like on your hypnogram in the morning [21,22,23,24]:
How to use your hypnogram without spiraling into analysis paralysis
Waking up to a poor sleep score and spending the next day convinced the night was a disaster, or obsessing over a single low deep-sleep reading and trying to "fix" it the following night through earlier bedtimes, supplements, or behavioral changes, is straight up “sleep score anxiety,” and we do not like this for you.
The anxiety is understandable, but it fundamentally misreads what wearable data is good for. The most important principle, supported consistently across the research literature and clinical guidance, is this: trust the trend, not the night.
A 2025 benchmark analysis by Terra Research stated this plainly: the real value of a sleep tracker lies in recognizing patterns over time, rather than obsessing over single-night accuracy [18]. Clinical guidance on consumer sleep trackers similarly advises clinicians to emphasize behavioral trends and multiday averages rather than nightly readings [4].
Why does this matter so much? Night-to-night variability in sleep-stage data from wearables is substantial. Variability can be caused by both genuine biological variation and measurement imprecision. A single night in which your device shows low deep sleep may reflect a true deficit, an algorithmic misclassification, a body-position artifact, or simply normal night-to-night fluctuation.
You cannot know which.
However, a trend of consistently low deep sleep over two to three weeks is worth paying attention to.
What your wearable may be getting wrong
We want so badly for technology to be perfect so we can trust it. But alas, even our smartest smart ring has failure modes worth noting.
A March 2025 study in SLEEP Advances tested the Apple Watch Series 8 alongside five other wrist-worn devices against in-lab polysomnography (PSG) and found that while some devices showed clinically acceptable accuracy for certain parameters, all showed significant differences from the holy grail of sleep measurement, the PSG.
These differences included total sleep time, sleep efficiency, and wake after sleep onset [13].
Because a PSG measures brain waves, and our cute little smart ring captures data from an accelerometer and heart rate rather than brain waves, it infers sleep stages from physiological proxies and frequently misclassifies N3 as lighter sleep.
Deep sleep is the most mislabeled stage. According to Apple’s own validation data, when the Apple Watch predicts “Core Sleep,” the true PSG stage is actually deep sleep 38% of the time [2].
REM fares better because heart rate variability during REM is distinctive enough to be detected reasonably well without an EEG. N1 is nearly invisible to wearables, which is acceptable since it is brief and functionally minor.
There is also an epoch-resolution problem: PSG scores sleep in 30-second windows, while most wearables use 1–5-minute windows, smearing brief stage transitions into adjacent categories.
Metrics worth trusting
Averages and trends over time.
Look at 7- and 30-day averages first. Most wearable apps display weekly and monthly summaries. These are the numbers to anchor on. A 30-day average deep sleep percentage below 10% or REM below 15% is more meaningful than any single night’s reading.
Hypnogram shapes, not just labels.
The overall architecture of your sleep, whether you descend into deeper stages and return in recognizable cycles, is more reliably captured than the specific stage labels. A hypnogram showing chaotic, fragmented transitions every night is more concerning than one showing smooth cycling with occasional mislabeling, which smart rings are notorious for doing.
Identify your personal patterns.
Does your sleep score reliably drop after alcohol? After a late dinner? After high-stress workdays? After exercise in the evening? Wearables are excellent at helping you detect your personal behavioral sensitivities and use them as a feedback tool for your own habits, not as a nightly report card.
Track wake after sleep onset (WASO).
This metric shows how long you were awake after initially falling asleep and is among the most reliably measured by wearables. Consistently high WASO (greater than 30 minutes) across multiple nights warrants attention and possibly a conversation with a clinician.
Don’t chase the score.
Optimizing behavior specifically to improve a wearable sleep score can be counterproductive, particularly if it leads to performance anxiety at bedtime. The behaviors that genuinely improve sleep (consistent sleep and wake times, limiting alcohol, managing evening light exposure, time-restricted eating, and addressing stress) will improve your average score over time. The nightly number is a byproduct, not the target.
Sleep and wake timing, every night.
Consistent timing across seven days is one of the strongest behavioral predictors of sleep quality and circadian health, and it is also the metric wearables measure most accurately.
I also dropped these same metrics into a convenient one-pager you can download and share.
The practical bottom line
Use your sleep data in the following order of trust:
Most reliable: Total sleep time, consistency of sleep and wake timing, and overall fragmentation patterns across weeks.
Directionally useful: Stage trends over time. If your REM or deep sleep consistently appears low across multiple weeks, it is worth exploring with a sleep specialist. Do not optimize nightly based on a single reading.
Treat with caution: Any single night’s stage breakdown. Architecture is more trustworthy than labels; trends across nights are far more trustworthy than any individual reading.
Happy sleeping, everyone.
──────────────────────────────
If this was useful, here’s where to go next:
→ You’re navigating chronic illness and want a clear roadmap: go here
→ You lead a clinic and want to bring this education to your patients: grab the sample curriculum here
→ You run a retreat and want to add science-backed depth to your program: go here
──────────────────────────────
References
Alblewi, S. M., & Mirghani, H. (2025). Chronotype’s effect on academic achievement and absence from classrooms and clinical sessions among clinical phase medical students. Frontiers in Psychology, 16, 1664598. https://doi.org/10.3389/fpsyg.2025.1664598
Apple Inc. (2025). Estimating sleep stages from Apple Watch (White paper, updated October 2025). https://www.apple.com/health/pdf/Estimating_Sleep_Stages_from_Apple_Watch_Oct_2025.pdf
Bartsch, U., & Bhatt, D. L. (2023). Emotional memory processing during REM sleep with implications for post-traumatic stress disorder. Journal of Neuroscience, 43(3), 433–448. https://doi.org/10.1523/JNEUROSCI.0590-22.2022
CHEST Physician. (2025, October). Using consumer sleep trackers in clinical practice. CHEST Physician. https://www.chestphysician.org/consumer-sleep-trackers-in-clinical-practice/
Cho, Y. W., Lee, J. H., Han, S. Y., & Lee, M. Y. (2024). Validity and reliability of the Korean version of reduced Morningness-Eveningness Questionnaire: Results from a general population-based sample. Journal of Korean Medical Science, 39(28), e257. https://doi.org/10.3346/jkms.2024.39.e257
Corbali, O., & Levey, A. I. (2025). Glymphatic system in neurological disorders and implications for brain health. Frontiers in Neurology, 16, 1543725. https://doi.org/10.3389/fneur.2025.1543725
Hilditch, C. J., Dorrian, J., & Banks, S. (2025). The linkage between chronotype, social jetlag, and responses to sleep inertia. Scientific Reports, 15, 12858. https://doi.org/10.1038/s41598-025-93057-7
Horne, J. A., & Ostberg, O. (1976). A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. International Journal of Chronobiology, 4(2), 97–110.
Huang, X., et al. (2024). Misalignment between circadian preference and accelerometer-derived actual sleep-wake cycle is associated with increased risk of cardiometabolic diseases: A prospective cohort study in UK Biobank. medRxiv. https://doi.org/10.1101/2024.06.28.24309628
Kiviniemi, V., Nedergaard, M., et al. (2025). Norepinephrine-mediated slow vasomotion drives glymphatic clearance during sleep. Cell, 188(1). https://doi.org/10.1016/j.cell.2024.11.027
Li, M., et al. (2025). Social jet lag and mental health outcomes: A systematic review and meta-analysis. Acta Psychologica. https://doi.org/10.1016/j.actpsy.2025.104954
Patel, A. K., Reddy, V., Shumway, K. R., & Araujo, J. F. (2024). Physiology, sleep stages. In StatPearls [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK526132/
Schyvens, A.-M., Peters, B., Van Oost, N. C., Aerts, J.-M., Masci, F., Neven, A., Dirix, H., Wets, G., Ross, V., & Verbraecken, J. (2024). Accuracy of Fitbit Charge 4, Garmin Vivosmart 4, and WHOOP versus polysomnography: Systematic review. JMIR mHealth and uHealth, 12, e52192. https://doi.org/10.2196/52192
Schyvens, A.-M., Peters, B., Van Oost, N. C., Aerts, J.-M., Masci, F., Neven, A., Dirix, H., Wets, G., Ross, V., & Verbraecken, J. (2025). A performance validation of six commercial wrist-worn wearable sleep-tracking devices for sleep stage scoring compared to polysomnography. SLEEP Advances, 6(2), zpaf021. https://doi.org/10.1093/sleepadvances/zpaf021
Sladek, M., Klusacek, J., Hamplova, D., & Sumova, A. (2023). Population-representative study reveals cardiovascular and metabolic disease biomarkers associated with misaligned sleep schedules. Sleep, 46(5), zsad037. https://doi.org/10.1093/sleep/zsad037
Slowik, J. M., Collen, J. F., & Yow, A. G. (2023). Physiology of sleep. In StatPearls [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK482512/
Stickgold, R. (2005). Sleep-dependent memory consolidation. Nature, 437(7063), 1272–1278. https://doi.org/10.1038/nature04286
Terra Research. (2025). Benchmarking wearable sleep data reliability. Terra Research. https://tryterra.co/research/sleep-tracking-accuracy
Xie, L., Kang, H., Xu, Q., Chen, M. J., Liao, Y., Thiyagarajan, M., O’Donnell, J., Christensen, D. J., Nicholson, C., Iliff, J. J., Takano, T., Deane, R., & Nedergaard, M. (2013). Sleep drives metabolite clearance from the adult brain. Science, 342(6156), 373–377. https://doi.org/10.1126/science.1241224
Zheng, N. S., Annis, J., Master, H., Han, L., Gleichauf, K., Ching, J. H., Nasser, M., Coleman, P., Desine, S., Ruderfer, D. M., Hernandez, J., Schneider, L. D., & Brittain, E. L. (2024). Sleep patterns and risk of chronic disease as measured by long-term monitoring with commercial wearable devices in the All of Us Research Program. Nature Medicine, 30(9), 2648–2656. https://doi.org/10.1038/s41591-024-03155-8
American Academy of Sleep Medicine. (2020). The AASM manual for the scoring of sleep and associated events: Rules, terminology and technical specifications (Version 2.6). American Academy of Sleep Medicine.
National Heart, Lung, and Blood Institute. (2024). Your guide to healthy sleep: The stages of sleep. National Institutes of Health. NHLBI Sleep Stages Overview
Sleep Foundation. (2024). Sleep stages: REM, NREM, and how they work. Sleep Foundation Sleep Architecture Review
Cleveland Clinic. (2023). Sleep cycles: Stages, how long they last, and why they matter. Cleveland Clinic Sleep Cycles Explanation
From a clinical perspective, when sleep stage distribution is off, what’s usually driving it; stress, circadian disruption, or metabolic health, and how can you tell which is affecting you?