

Circadian health in clinical practice
A practical framework for assessing biological timing, identifying circadian disruption, and applying timing-based interventions


Part 2 of 2
In Part 1, we explored how the body tells time.
We followed the circadian signal from the retina to the suprachiasmatic nucleus, through the transcription-translation feedback loop, and into the peripheral tissues that coordinate metabolism, immune function, hormone secretion, and cellular repair.
Together, these systems create an internal timing network that allows physiology to anticipate predictable environmental demands rather than simply react to them as they occur.
The obvious question is whether any of this matters in clinical practice.
For much of the history of modern medicine, circadian biology has remained largely confined to sleep medicine, chronobiology laboratories, and shift-work research.
Clinicians may learn that cortisol follows a diurnal rhythm or that melatonin rises at night, but circadian timing has rarely been incorporated into routine patient assessment in the same way that nutrition, physical activity, blood pressure, or glycemic control have.
That is beginning to change.
The 2025 American Heart Association scientific statement on circadian health placed sleep timing regularity, meal timing, light exposure, and physical activity timing alongside more familiar cardiometabolic risk factors, framing them as modifiable determinants of health rather than lifestyle preferences.
This represents a meaningful shift. Timing is increasingly being viewed not as background context, but as a physiological variable worthy of clinical attention.
The challenge, of course, is practical.
What exactly are we assessing? How do we identify circadian disruption? What can we measure?
And perhaps most importantly, what do we do with the information once we find it?
Circadian health as a clinical construct
One reason circadian medicine has struggled to gain traction clinically is that the field has historically lacked a practical framework.
Most clinicians are comfortable assessing blood pressure, glycemic control, body composition, physical activity, sleep duration, or dietary quality. Circadian health is less intuitive because it cannot be reduced to a single laboratory value or biomarker.
Historically, circadian assessment focused primarily on phase.
What time is the patient’s clock?
While phase remains important, emerging frameworks suggest that circadian health is more appropriately viewed as a multidimensional construct encompassing phase, amplitude, regularity, and synchronization.
These four domains provide a useful starting point for clinical assessment.
Phase refers to the timing of the circadian system relative to clock time. It determines when an individual reaches biological morning, biological evening, and biological night.
Chronotype is one expression of phase.
Some individuals naturally function earlier, while others function later. The question is not whether one chronotype is superior to another, but whether an individual’s behavioral schedule aligns with their biological timing.
Amplitude describes the strength of circadian oscillations. Healthy systems exhibit robust daily variation in hormone secretion, body temperature, alertness, activity, and metabolic function. With aging, chronic disease, irregular schedules, and prolonged circadian disruption, these rhythms often become flattened.
Regularity refers to the consistency of timing signals across days. Sleep timing, meal timing, light exposure, and activity patterns all contribute. A patient who sleeps, eats, and exercises at roughly the same times each day provides the circadian system with predictable information. A patient whose schedule varies substantially between weekdays and weekends does not.
Synchronization refers to the degree of agreement among timing signals and physiological systems. Are sleep, light exposure, feeding behavior, and activity reinforcing one another? Or are they providing conflicting information?
This concept captures the phenomenon of internal desynchrony described in Part 1, where central and peripheral clocks drift into discordant phase relationships despite continuing to function independently.
Together, these domains move circadian assessment beyond a simple discussion of sleep duration and toward a broader evaluation of temporal physiology.
What circadian disruption looks like in practice
The challenge for clinicians is recognizing when timing may be contributing to the presentation of familiar clinical concerns.
Consider the patient with a delayed chronotype who wakes at 5:30 every morning for work despite naturally falling asleep after midnight. Their laboratory values may initially appear normal. Sleep duration may even seem adequate. Yet they spend years functioning against their biological timing.
Or consider the retiree whose decades-long schedule disappears almost overnight. Wake times become inconsistent. Meals drift throughout the day. Activity patterns become less predictable. Sleep quality gradually deteriorates despite having complete control over the schedule.
In both cases, timing signals become weaker, less consistent, or less synchronized.
Shift workers represent perhaps the most obvious example. Rotating schedules repeatedly force misalignment between the light-dark cycle, behavioral timing, and intrinsic circadian phase.
Epidemiological studies consistently associate shift work with increased risk of obesity, type 2 diabetes, cardiovascular disease, certain cancers, and all-cause mortality.
However, most circadian disruption encountered in clinical practice is considerably less dramatic.
Social jet lag may be more common than shift work. A patient maintains one schedule during the workweek and another on weekends, shifting biological timing back and forth every seven days.
Menopause represents another population in whom circadian assessment may prove valuable. Changes in hormone regulation influence thermoregulation, sleep continuity, circadian stability, and vulnerability to environmental timing cues. The symptoms are often attributed solely to endocrine changes, yet circadian disruption may compound the clinical picture.
Frequent travelers provide a final example. Repeated phase shifts challenge the system’s ability to maintain alignment, particularly when travel crosses multiple time zones and recovery periods are limited.
Measuring circadian timing
If circadian timing matters, how do we assess it?
The gold standard remains dim-light melatonin onset (DLMO), which measures the timing of endogenous melatonin secretion under controlled lighting conditions [6]. From a research perspective it is the benchmark; from a clinical perspective it is largely impractical, since few clinicians are positioned to collect serial evening saliva samples under carefully controlled lighting.
As a result, circadian medicine currently relies on a combination of direct and indirect assessments.
Chronotype questionnaires remain among the simplest tools available. While imperfect, they provide useful information regarding an individual’s preferred timing of sleep and activity.
Clinical history remains surprisingly powerful. Questions regarding sleep timing, wake timing, shift-work exposure, meal schedules, travel patterns, and day-to-day variability often reveal substantial circadian disruption before any formal testing is performed.
Actigraphy provides an objective assessment of rest-activity rhythms over extended periods. Unlike a single night of sleep testing, actigraphy captures timing, regularity, and behavioral patterns across days or weeks. This longitudinal perspective is often more valuable for circadian assessment than a single physiological snapshot.
Wearable devices are increasingly expanding these capabilities. While consumer devices should not be mistaken for validated circadian assessments, they provide unprecedented access to longitudinal behavioral data. Sleep timing, activity rhythms, temperature patterns, and regularity metrics can all contribute useful information when interpreted appropriately.
One metric receiving increasing attention is the Sleep Regularity Index (SRI). Unlike traditional sleep measures that focus primarily on duration, the SRI quantifies consistency in sleep-wake behavior across days.
Recent evidence suggests that sleep regularity may be independently associated with cardiometabolic outcomes, highlighting the importance of timing stability in addition to sleep quantity.
Importantly, none of these measures fully captures circadian health. They are proxies, and the field remains limited by our ability to measure phase, amplitude, and synchronization efficiently in real-world settings.
Circadian timing as a therapeutic target
Once timing becomes part of the assessment, the mechanisms that drive the system also become levers for intervention.
Light remains the dominant zeitgeber for the central clock. Morning light exposure strengthens entrainment, reinforces synchronization, and helps anchor circadian phase to the external environment. Evening light, particularly short-wavelength light, produces the opposite effect.
Meal timing functions as one of the strongest zeitgebers for peripheral metabolic tissues. The liver, pancreas, gastrointestinal tract, and adipose tissue all respond to feeding schedules, and the gut microbiome itself follows a daily rhythm shaped by when we eat.
Irregular or prolonged eating windows can uncouple metabolic timing from central circadian signals, whereas structured meal timing may help restore synchronization.
Physical activity also functions as a timing signal. Through changes in cellular energy status, calcium signaling, and metabolic demand, exercise influences peripheral clock function and may reinforce circadian organization depending on when it occurs.
Sleep regularity may ultimately prove one of the most practical levers of all. Consistent wake times strengthen the relationship between light exposure, activity, feeding behavior, and sleep, reinforcing multiple timing systems simultaneously.
Chronotherapy extends these concepts into pharmacology. Blood pressure regulation, inflammatory signaling, hormone secretion, and drug metabolism all exhibit circadian variation.
As evidence accumulates, aligning medication timing with biological timing may improve efficacy while reducing adverse effects. The principle now reaches into oncology, where chrono-immunotherapy is being explored as a way to time treatment to the rhythms of the immune system.
Why circadian medicine is slow to reach the clinic
Given the breadth of evidence linking circadian disruption to cardiometabolic disease, immune dysfunction, neurodegeneration, psychiatric illness, and cancer, an obvious question emerges: why has circadian medicine been so slow to enter routine practice?
The primary barrier is measurement.
Modern medicine is built around quantifiable biomarkers. Blood pressure, glucose, lipids, inflammatory markers, imaging findings, and pathology results can all be measured directly and incorporated into clinical decision-making.
Circadian phase is harder. As noted above, gold-standard techniques such as DLMO, constant routine protocols, and laboratory-based phase mapping remain largely confined to research settings and specialist centers.
Although wearable-derived metrics, metabolomic approaches, and AI-assisted circadian phenotyping are advancing rapidly, scalable clinical tools remain limited.
A second barrier is education. Most physicians receive little formal training in circadian biology outside of sleep medicine. As a result, concepts such as chronotype, phase, amplitude, and internal desynchrony are rarely incorporated into routine history taking, despite growing evidence that these factors influence disease risk and treatment response across specialties.
A third is that circadian medicine does not fit neatly within traditional specialty boundaries. Cardiologists encounter circadian influences on blood pressure regulation, thrombosis risk, and cardiovascular events.
Endocrinologists encounter circadian regulation of glucose metabolism and insulin sensitivity. Neurologists and psychiatrists routinely manage disorders characterized by disrupted sleep-wake and activity rhythms. Rheumatologists observe daily variation in inflammatory symptoms, and oncologists are increasingly exploring chronotherapy and chrono-immunotherapy.
Timing influences each of these fields, yet ownership of the topic remains fragmented, so the challenge is translating that biology into practical clinical workflows.
What clinicians can do today
Comprehensive circadian phenotyping remains largely a research endeavor. But physicians do not need access to a chronobiology laboratory to begin applying circadian principles. The tools described above condense into three practical steps:
assess timing,
incorporate chronotype, and
treat timing as a therapeutic variable.
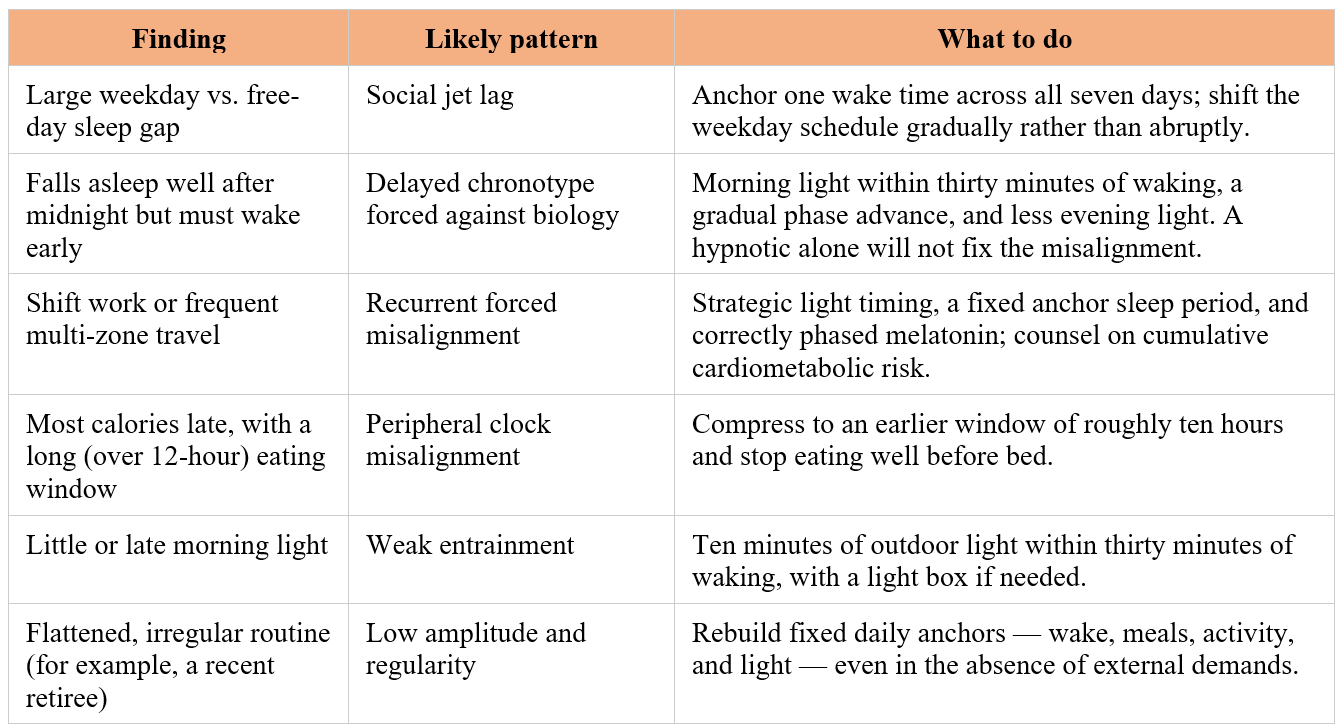
The first step is simply assessing timing.
For patients presenting with sleep complaints, metabolic instability, hypertension, obesity, mood disorders, fatigue, variable treatment response, or shift-work exposure, a brief circadian history often reveals substantial disruption before any formal testing is considered. Six questions require no equipment:
What time do you naturally become sleepy when you have no obligations the next morning?
What time do you naturally wake without an alarm?
How different are your sleep schedules on workdays and free days?
Do you perform shift work or frequently travel across time zones?
When do you consume most of your calories?
When do you receive your first significant light exposure of the day?
The second step is incorporating chronotype into clinical reasoning.
Validated questionnaires such as the Munich Chronotype Questionnaire (MCTQ) and the Morningness-Eveningness Questionnaire (MEQ) can be completed in minutes and provide practical estimates of circadian preference. Both are available at the end of this article.
When a questionnaire is not at hand, understanding a patient’s mid-sleep on free days (the midpoint of sleep on non-working days, corrected for accumulated sleep debt) is the most reproducible proxy and tracks dim-light melatonin onset reasonably well across populations.
Two facts make chronotype more useful. It is highly heritable and shifts predictably across the lifespan, moving toward eveningness through adolescence, partially reversing in the mid-thirties, and advancing again in older age. So the right time for an intervention changes with a patient’s stage of life. Because it is roughly 50% heritable, it means a family history of extreme early or late sleep timing is clinically informative.
Chronotype is not a substitute for formal phase assessment, but it offers a useful framework for understanding how a patient’s biological timing interacts with work schedules, treatment plans, and behavioral recommendations.
The third step is treating timing as a therapeutic variable.
The mechanisms outlined earlier translate directly into interventions that can be implemented immediately and at no cost. Behavioral levers come first because they are the most accessible:
Morning light. Roughly 10 minutes of outdoor light within 30 minutes of waking reinforces SCN entrainment and anchors circadian phase. It is a zero-cost, first-line measure for delayed phase, seasonal mood symptoms, jet lag, and shift-work complaints.
Consistent sleep and wake times across both workdays and free days, which reduces social jet lag and strengthens alignment regardless of total sleep obtained.
An early, structured eating window of roughly 10 hours, avoiding prolonged late-evening eating, which improves peripheral clock synchronization and glucose tolerance independent of caloric intake.
Exercise timed with phase in mind: morning or early-afternoon activity generally advances the clock, while vigorous late-evening exercise can delay it. This is a useful distinction in patients with significant phase delay.
Melatonin deserves separate mention because it is so often misused. It is a chronobiotic (phase-shifting agent), not a sedative. Given at the correct phase (early evening for delayed sleep phase, early morning for advanced phase), it produces meaningful shifts in the intended direction; given at the wrong phase, or as a high bedtime dose without regard to phase, it can worsen misalignment or do nothing at all. The familiar habit of prescribing 5–10 mg at bedtime as a sleep aid is biologically irrational for most patients with phase-based complaints.
Pharmacologic timing, chronotherapy, extends these principles into prescribing. Drug bioavailability, receptor expression, enzyme activity, and tissue sensitivity all vary by circadian phase, so the same dose given at different times can differ in both efficacy and tolerability. The applications below have the most mature evidence:
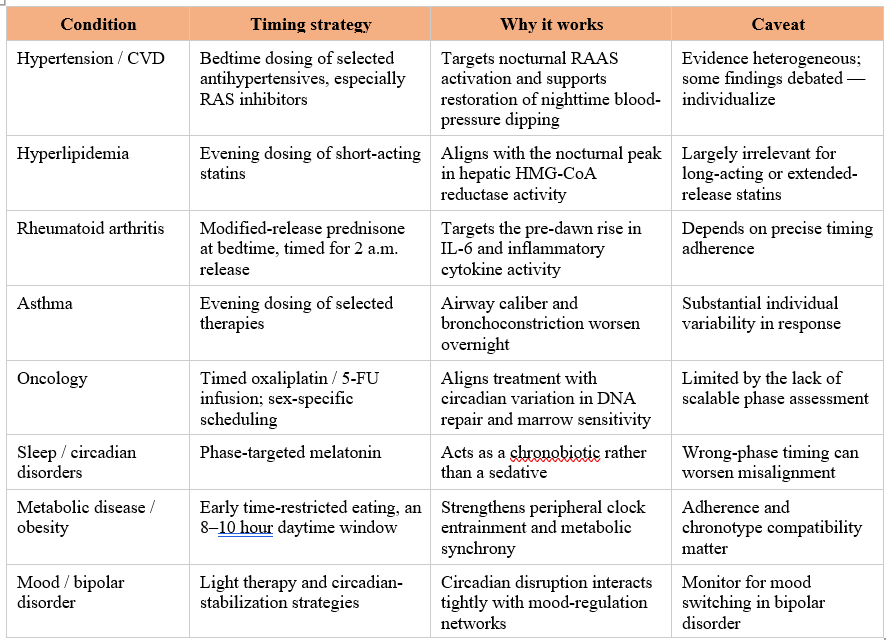
[Abbreviations: RAS, renin–angiotensin system; RAAS, renin–angiotensin–aldosterone system; IL-6, interleukin-6; 5-FU, 5-fluorouracil]
These strategies should not be applied as universal rules. The evidence base is still uneven. Antihypertensive dosing is the clearest example: the Hygia Chronotherapy Trial, a Spanish study of roughly 19,000 patients, reported a striking 45% reduction in cardiovascular events with bedtime dosing, but the finding was never independently replicated.
Many other chronotherapy trials are similarly limited by small samples and inconsistent phase assessment. More fundamentally, the biological effect of any timing intervention depends on when it occurs relative to the patient’s internal clock, not the clock on the wall.
Assess chronotype before prescribing a window; forcing a late chronotype onto an early schedule without gradual phase-shifting can deepen desynchrony rather than resolve it.
Chronotype, age, occupation, and environment all shape what counts as well-timed.
Conclusion
Across these two parts, the argument has been straightforward. The body keeps time, that timing is biologically consequential, and the consequences reach into nearly every organ system clinicians already manage.
What has been missing is not the science but the translation.
Circadian phase has remained difficult to measure at scale, training has lagged the evidence, and the topic has fallen between specialties rather than belonging to any one of them.
Yet none of that prevents a clinician from beginning today.
A short circadian history, a chronotype questionnaire, and a handful of timing-based interventions can be incorporated into existing practice without new equipment or referral pathways. As wearable data, metabolomic markers, and computational phenotyping mature, the measurement gap that has held the field back is likely to narrow.
Circadian medicine is unlikely to become a separate specialty. More likely, it will become an additional dimension of clinical assessment, taking its place alongside blood pressure, nutrition, physical activity, and sleep itself, asking of each patient not only what is happening, but when.
Tools mentioned in this piece
The screening questions and timing interventions above are collected in a one-page Circadian consult quick-reference (free to download and share).
The two validated chronotype questionnaires are copyrighted instruments, so I can't reproduce them here but both are freely obtainable:
MCTQ (Munich Chronotype Questionnaire) — thewep.org/documentations/mctq; free to use, with permission requested from the authors.
MEQ (Morningness-Eveningness Questionnaire) — free self-assessment at the Center for Environmental Therapeutics, cet.org.
References
Campbell-Galland A, Bafna A, Jagannath A. The molecular circadian clock: From fundamental mechanisms to therapeutic promise in neurological disorders. Adv Drug Deliv Rev. 2025 Sep;224:115653. doi: 10.1016/j.addr.2025.115653. Epub 2025 Jul 12. PMID: 40659217.
Bautista J, Ojeda-Mosquera S, Ordóñez-Lozada D, López-Cortés A. Peripheral clocks and systemic zeitgeber interactions: from molecular mechanisms to circadian precision medicine. Front Endocrinol (Lausanne). 2025 May 29;16:1606242. doi: 10.3389/fendo.2025.1606242. PMID: 40510487; PMCID: PMC12158691.
Knutson KL, Dixon DD, Grandner MA, Jackson CL, Kline CE, Maher L, Makarem N, Martino TA, St-Onge MP, Johnson DA; American Heart Association Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; and Council on Lifelong Congenital Heart Disease and Heart Health in the Young. Role of Circadian Health in Cardiometabolic Health and Disease Risk: A Scientific Statement From the American Heart Association. Circulation. 2025 Nov 25;152(21):e408-e419. doi: 10.1161/CIR.0000000000001388. Epub 2025 Oct 28. PMID: 41147137.
Liu Y, Huo R, Zhang EE. Evolving perspectives on the molecular and neural foundations of mammalian circadian rhythms. Trends Neurosci. 2025 Nov;48(11):904-918. doi: 10.1016/j.tins.2025.09.009. Epub 2025 Oct 9. PMID: 41073229.
Laothamatas I, Rasmussen ES, Green CB, Takahashi JS. Metabolic and chemical architecture of the mammalian circadian clock. Cell Chem Biol. 2023 Sep 21;30(9):1033-1052. doi: 10.1016/j.chembiol.2023.08.014. Epub 2023 Sep 13. PMID: 37708890; PMCID: PMC10631358.
Lecacheur M, Ammerlaan DJM, Dierickx P. Circadian rhythms in cardiovascular (dys)function: approaches for future therapeutics. NPJ Cardiovasc Health. 2024 Sep 23;1(1):21. doi: 10.1038/s44325-024-00024-8. PMID: 41776061; PMCID: PMC12912364.
Fagiani, F., Di Marino, D., Romagnoli, A. et al.Molecular regulations of circadian rhythm and implications for physiology and diseases. Sig Transduct Target Ther 7, 41 (2022). https://doi.org/10.1038/s41392-022-00899-y
Mendoza J. Brain circadian clocks timing the 24h rhythms of behavior. NPJ Biol Timing Sleep. 2025 Mar 22;2(1):13. doi: 10.1038/s44323-025-00030-8. PMID: 41776262; PMCID: PMC12912386.
Morin R, Forest G, Imbeault P. Circadian rhythms revealed: unraveling the genetic, physiological, and behavioral tapestry of the human biological clock and rhythms. Front Sleep. 2025 Jun 4;4:1544945. doi: 10.3389/frsle.2025.1544945. PMID: 41425175; PMCID: PMC12713876.
Nagayach A, Bhaskar R, Ghosh S, M D, Abomughaid MM, Han SS, Singh KK, Almutary AG, Chaudhary K, Atteri S, Chauhan AS, Jha NK, Sinha JK. Interplay between circadian rhythm, ageing and neurodegenerative disorder. Open Biol. 2025 Jul;15(7):240161. doi: 10.1098/rsob.240161. Epub 2025 Jul 23. PMID: 40695322.
Satyam SM, Prabhakar S, El-Tanani M, Bhongade B, Wali AF, Rangraze IR, Matalka IIA, El-Tanani Y, Rizzo M, Ispas S, Ilias I, Paczkowska A, Maggio V, Hoffmann K. Chronopharmacology-Driven Precision Therapies for Time-Optimized Cardiometabolic Disease Management. Biology (Basel). 2026 Jan 28;15(3):241. doi: 10.3390/biology15030241. PMID: 41677713; PMCID: PMC12896478.
Kaşkal M, Sevim M, Ülker G, Keleş C, Bebitoğlu BT. The clinical impact of chronopharmacology on current medicine. Naunyn Schmiedebergs Arch Pharmacol. 2025 Jun;398(6):6179-6191. doi: 10.1007/s00210-025-03788-7. Epub 2025 Jan 10. PMID: 39792169; PMCID: PMC12125046.
Bedont JL, Iascone DM, Sehgal A. The Lineage Before Time: Circadian and Nonclassical Clock Influences on Development. Annu Rev Cell Dev Biol. 2020 Oct 6;36:469-509. doi: 10.1146/annurev-cellbio-100818-125454. PMID: 33021821; PMCID: PMC10826104.
Patton AP, Hastings MH. The Mammalian Circadian Time-Keeping System. J Huntingtons Dis. 2023;12(2):91-104. doi: 10.3233/JHD-230571. PMID: 37125558; PMCID: PMC7614869.
Young MJ, Heanue S, Kanki M, Moneghetti KJ. Circadian disruption and its impact on the cardiovascular system. Trends Endocrinol Metab. 2025 Sep;36(9):842-854. doi: 10.1016/j.tem.2024.11.010. Epub 2024 Dec 19. PMID: 39706759.
Zheng B, Wang L, Sun S, Yuan X, Liang Q. The molecular interplay between the gut microbiome and circadian rhythms: an integrated review. Front Microbiol. 2025 Dec 5;16:1712516. doi: 10.3389/fmicb.2025.1712516. PMID: 41425940; PMCID: PMC12715601.
Özdemir BC, Bill R, Okyar A, Scheiermann C, Hayoz S, Olivier T. Chrono-immunotherapy as a low-hanging fruit for cancer treatment? A call for pragmatic randomized clinical trials. J Immunother Cancer. 2025 Mar 3;13(3):e010644. doi: 10.1136/jitc-2024-010644. PMID: 40032603; PMCID: PMC11877229.
Romero-Franco, A., Checa-Rodríguez, C., Jimeno, S. et al. Circadian regulation of homologous recombination by cryptochrome1-mediated dampening of DNA end resection. Nat Commun 16, 10802 (2025). https://doi.org/10.1038/s41467-025-65854-1
Lévi FA, Okyar A, Hadadi E, Innominato PF, Ballesta A. Circadian Regulation of Drug Responses: Toward Sex-Specific and Personalized Chronotherapy. Annu Rev Pharmacol Toxicol. 2024;64:89–114. doi: 10.1146/annurev-pharmtox-051920-095416
 | A guest post by
|
This is a great reminder that when we do things can be just as important as what we do. Small, consistent routines are often easier to maintain and can support better long-term health.
Excellent article!
There's also a political aspect to circadian health, and a science-backed movement to make "Standard Time" permanent, instead of subjecting people to the disruption of twice-yearly clock changes.
https://drmick.substack.com/p/living-in-sync-with-sunlight